
 Since I learned in April 2020 that transmission of covid was mainly via extremely small aerosols, I have regarded face masks as a placebo: they are to aerosols what garden gates are to mosquitoes. Yet, placebos have a role so I wasn’t too against them and willing to have my assessment overturned by new insights. After all, face masks might not stop aerosols, but they made many people feel better and might unexpectedly work in some other way against covid, such as by changing behaviour or changing the way the air flows into noses, or whatever. 16 months later, I am more against them because a multi-billion dollar industry has arisen that thrives on creating a mask-waste mountain and is thus heavily invested in their continued use, just as the industry of hand sanitizers, tests, and others. I personally found masks a nuisance to wear and an overt sign of submission. I have a like-minded friend in Sydney going around Sydney shops with a guy fawkes mask as a quiet symbol of defiance against compulsory masks.
Since I learned in April 2020 that transmission of covid was mainly via extremely small aerosols, I have regarded face masks as a placebo: they are to aerosols what garden gates are to mosquitoes. Yet, placebos have a role so I wasn’t too against them and willing to have my assessment overturned by new insights. After all, face masks might not stop aerosols, but they made many people feel better and might unexpectedly work in some other way against covid, such as by changing behaviour or changing the way the air flows into noses, or whatever. 16 months later, I am more against them because a multi-billion dollar industry has arisen that thrives on creating a mask-waste mountain and is thus heavily invested in their continued use, just as the industry of hand sanitizers, tests, and others. I personally found masks a nuisance to wear and an overt sign of submission. I have a like-minded friend in Sydney going around Sydney shops with a guy fawkes mask as a quiet symbol of defiance against compulsory masks.
I want to share two external reviews on masks of two different groups I have been following. One is a group of largely retired UK doctors who assembled in 2020: the HART group that looks at all the medical science around covid. The people involved in that group write on personal title, so one knows who the advice is from, which is a big plus. The second is a pre-existing’ Swiss policy research’ group formed in 2016. It is a bit like the research version of wikileaks and seems to have found its origin largely in concerns for press freedom and suspicion of the CIA, which is why its contributors are anonymous (which I understand, but dont like, particularly not as a sole source of information). SWPR took it upon itself early on to wade through the science of covid so as to come to its own assessment.
I have found the combination of them useful. SWPR is not so good in understanding the models or being consistent about what explains covid-outcomes, but is good at classic medical stuff (treatments, trials) and media manipulation. The HART group is good on covid measurement issues, medical organizational matters, and has better modelers on their team, but it largely stays away from political economy and is less prepared to venture guesses about origins and such. Yet, both have taken reasonable lines on things for which there is little doubt. Both those sources for instance say vaccines reduce covid severity. These sources have not always agreed the last 18 months and I have noted technical issues in areas I have particular expertise where they didn’t quite understand what some sophisticated empirical studies were saying, but I have learned to lean on them for useful summary takes. I haven’t detected an obvious bias. Here is what the HART people say about masks (https://www.hartgroup.org/masks/):
Contrary to the Government message that it ‘follows the science’, the sudden change in advice by the WHO was not based on any new, high-quality scientific studies. By summer 2020, there was substantial evidence that non-medical masks for the general public did not reduce the transmission of respiratory viruses. A review of 14 controlled studies had concluded that masks did not significantly lessen the spread of seasonal ‘flu in the community.1 A Norwegian Institute for Public Health review found that non-medical masks achieve no benefit for healthy individuals, particularly when viral prevalence is low.1 From a common sense angle, scientists had argued that cloth masks contain perforations that are far too big to act as a viral barrier and therefore ‘offer zero protection against COVID-19’.1
Inevitably, the public often wear masks incorrectly, or improperly handle them when putting them on, or removing them, constituting an additional infection hazard. There has been recognition of this contamination risk in the scientific literature1 and other researchers have cautioned against the use of cloth face coverings.1 Potential harms to the wearer include exhaustion, headaches, fatigue and dehydration.1 Some doctors have suggested an increased risk of pneumonia.1 Furthermore, the widely varying physical characteristics of the face coverings used by people in the community, that are not standardised for material, fit, length of wearing, changes after washing and drying, and disposal, means that laboratory research on mask efficacy cannot be generalised to real-world situations.
With particular reference to COVID-19, the only large randomised controlled trial exploring the benefits of adopting face coverings in the community found that masks (even the surgical variety) did not result in a significant reduction in infection risk for the wearer.1 A detailed analysis1 of all research investigations, including those purported to suggest that masks might achieve some benefits, led to the view that there is ‘little to no evidence’ that cloth masks in the general population are effective.
Masks impair verbal communication, render lip-reading impossible for the deaf, and stymie emotional expression, the latter effect potentially constituting a gross impediment to children’s social development. Acting as a crude, highly visible reminder that danger is all around, face coverings are fuelling widespread, irrational fear.
Wearing a mask will heighten the distress of many people with existing mental health problems and may trigger ‘flashbacks’ for those historically traumatised by physical and/or sexual abuse. Sadly, going without a mask (even as a means of avoiding psychological distress) can often attract harassment and further victimisation. In response to this, ‘exemption lanyards’ have been developed, which further stigmatise those who cannot wear face coverings due to health conditions or previous trauma.
Note that this is their summary conclusion, which did not go over the more positive studies that one would like to see discussed. So below is what the Swiss policy people have just said about masks (https://swprs.org/face-masks-evidence/), whereby I only repeat their take-aways on various studies (both for and against). They have put their conclusions more starkly elsewhere, but here I basically stick to their literature analysis.
So far, most studies found little to no evidence for the effectiveness of face masks in the general population, neither as personal protective equipment nor as a source control.
- A May 2020 meta-study on pandemic influenza published by the US CDC found that face masks had no effect, neither as personal protective equipment nor as a source control. (Source)
- A Danish randomized controlled trial with 6000 participants, published in the Annals of Internal Medicine in November 2020, found no statistically significant effect of high-quality medical face masks against SARS-CoV-2 infection in a community setting. (Source)
- A large randomized controlled trial with close to 8000 participants, published in October 2020 in PLOS One, found that face masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection.” (Source)
- A February 2021 review by the European CDC found no high-quality evidence supporting the effectiveness of non-medical and medical face masks in the community. Furthermore, the European CDC advised against the use of FFP2/N95 masks by the general public. (Source)
- A July 2020 review by the Oxford Centre for Evidence-Based Medicine found that there is no evidence for the effectiveness of face masks against virus infection or transmission. (Source)
- A November 2020 Cochrane review found that face masks did not reduce influenza-like illness (ILI) cases, neither in the general population nor in health care workers. (Source)
- An April 2020 review by two US professors in respiratory and infectious disease from the University of Illinois concluded that face masks have no effect in everyday life, neither as self-protection nor to protect third parties (so-called source control). (Source)
- An article in the New England Journal of Medicine from May 2020 came to the conclusion that face masks offer little to no protection in everyday life. (Source)
- A 2015 study in the British Medical Journal BMJ Open found that cloth masks were penetrated by 97% of particles and may increase infection risk by retaining moisture or repeated use. (Source)
- An August 2020 review by a German professor in virology, epidemiology and hygiene found that there is no evidence for the effectiveness of face masks and that the improper daily use of masks by the public may in fact lead to an increase in infections. (Source)
Additional aspects
- There is increasing evidence that the novel coronavirus is transmitted, at least in indoor settings, not only by droplets but also by smaller aerosols. However, due to their large pore size and poor fit, most masks cannot filter out aerosols (see video analysis below): over 90% of aerosols penetrate or bypass the mask and fill a medium-sized room within minutes.
- The WHO admitted to the BBC that its June 2020 mask policy update was due not to new evidence but “political lobbying”: “We had been told by various sources WHO committee reviewing the evidence had not backed masks but they recommended them due to political lobbying. This point was put to WHO who did not deny.” (D. Cohen, BBC Medical Corresponent).
- To date, the only randomized controlled trial (RCT) on face masks against SARS-CoV-2 infection in a community setting found no statistically significant benefit (see above). However, three major journals refused to publish this study, delaying its publication by several months.
- An analysis by the US CDC found that 85% of people infected with the new coronavirus reported wearing a mask “always” (70.6%) or “often” (14.4%). Compared to the control group of uninfected people, always wearing a mask did not reduce the risk of infection.
- Researchers from the University of Minnesota found that the infectious dose of SARS-CoV-2 is just 300 virions (virus particles), whereas a single minute of normal speaking may generate more than 750,000 virions, making face masks unlikely to prevent an infection.
- In the US state of Kansas, the 90 counties without mask mandates had lower coronavirus infection rates than the 15 counties with mask mandates. To hide this fact, the Kansas health department tried to manipulate the official statistics and data presentation.
- Contrary to common belief, studies in hospitals found that the wearing of a medical mask by surgeons during operations didn’t reduce post-operative bacterial wound infections in patients.
- During the notorious 1918 influenza pandemic, the use of face masks among the general population was widespread and in some places mandatory, but they made no difference.
- The initially low coronavirus infection rate in some Asian countries was not due to masks, but due to very rapid border controls. For instance, Japan, despite its widespread use of face masks, had experienced its most recent influenza epidemic just one year prior to the covid pandemic.
- Early in the pandemic, the advocacy group “masks4all” argued that Czechia had few infections thanks to the early use of masks. In reality, the coronavirus simply hadn’t engulfed Eastern Europe yet; a few months later, Czechia had one of the highest infection rates in the world.
Studies claiming face masks are effective
Some recent studies argued that face masks are indeed effective against the new coronavirus and could at least prevent the infection of other people. However, most of these studies suffer from poor methodology and sometimes show the opposite of what they claim to show.
Typically, these studies ignore the effect of other measures, the natural development of infection rates, changes in test activity, or they compare places with different epidemiological conditions. Studies performed in a lab or as a computer simulation often aren’t applicable to the real world.
An overview:
- A meta-study in the journal Lancet, commissioned by the WHO, claimed that masks “could” lead to a reduction in the risk of infection, but the studies considered mainly N95 respirators in a hospital setting, not cloth masks in a community setting, the strength of the evidence was reported as “low”, and experts found numerous flaws in the study. Professor Peter Jueni, epidemiologist at the University of Toronto, called the WHO study “essentially useless”.
- A study in the journal PNAS claimed that masks had led to a decrease in infections in three global hotspots (including New York City), but the study did not take into account the natural decrease in infections and other simultaneous measures. The study was so flawed that over 40 scientists recommended that the study be withdrawn.
- A US study claimed that US counties with mask mandates had lower Covid infection and hospitalization rates, but the authors had to withdraw their study as infections and hospitalizations increased in many of these counties shortly after the study was published.
- A German study claimed that the introduction of mandatory face masks in German cities had led to a decrease in infections. But the data did not support this claim: in some cities there was no change, in others a decrease, in others an increase in infections (see graph below). The city of Jena was an ‘exception’ only because it simultaneously introduced the strictest quarantine rules in Germany, but the study did not mention this.
- A Canadian study claimed that countries with mandatory masks had fewer deaths than countries without mandatory masks. But the study compared countries with very different demographic structures and covered only the first few weeks of the pandemic.
- A review by the University of Oxford claimed that face masks are effective, but it was based on studies about SARS-1 and in health care settings, not in community settings.
- A review by members of the lobby group ‘Masks for All’, published in the journal PNAS, claimed that masks are effective as a source control against aerosol transmission in the community, but the review provided no real-world evidence supporting this proposition.
- A study published in Nature Communications in June 2021 claimed that masks reduced the risk of infection by 62%, but the study relied on numerous questionable modelling assumptions and on self-reported online survey results, not on actual measurements.
Risks associated with face masks
Wearing masks for a prolonged period of time may not be harmless, as the following evidence shows:
- The WHO warns of various “side effects” such as difficulty breathing and skin rashes.
- Tests conducted by the University Hospital of Leipzig in Germany have shown that face masks significantly reduce the resilience and performance of healthy adults.
- A German psychological study with about 1000 participants found “severe psychosocial consequences” due to the introduction of mandatory face masks in Germany.
- The Hamburg Environmental Institute warned of the inhalation of chlorine compounds in polyester masks as well as problems in connection with face mask disposal.
- The European rapid alert system RAPEX has already recalled 70 mask models because they did not meet EU quality standards and could lead to “serious risks”.
- A study by the University of Muenster in Germany found that on N95 (FFP2) masks, Sars-CoV-2 may remain infectious for several days, thus increasing the risk of self-contamination.
- In China, several children who had to wear a mask during gym classes fainted and died; the autopsies found a sudden cardiac arrest as the probable cause of death. In the US, a car driver wearing an N95 (FFP2) mask fainted and crashed due to CO2 intoxication.
Conclusion
Face masks in the general population might be effective, at least in some circumstances, but there is currently little to no evidence supporting this proposition. If the coronavirus is indeed transmitted via indoor aerosols, face masks are unlikely to be protective. Health authorities should therefore not assume or suggest that face masks will reduce the rate or risk of infection.
Postscript (August 2021)
A long-term analysis shows that infections have been driven primarily by seasonal and endemic factors, whereas mask mandates and lockdowns have had no discernible impact. 2
Conclusion (mine)
I can see the point of advocating a low-cost placebo even if it is unlikely to help and not supported by much science. So up till now I have not been too bothered. But the role of the mask industry in the political economy of covid is making me reconsider the damage that the mask-mandates are doing. The placebo is starting to look more and more costly. In such a circumstance, advocating masks under the essential argument that ‘they might help and it has not yet been proven they do not’ is no longer reasonable because that argument can be used for anything, from garlic necklaces to voodoo dolls. Given the lock-in effect by mask producers (and their waste-mountain effects), I think there should now be pretty solid evidence of strongly beneficial effects in order to advocate them. The onus of proof is hence on their adherents.
My main take home message to readers is to take the two sources of external summary views (the hartgroup and swpr) seriously. They cannot be censored by any internet giant. I have so far not found them to have an outrageous take on anything.
Probably the biggest RCT on masks has just been released, a study from Sri Lanka. Let us go over it carefully to see what it truly tells us about masks because I bet this study will be abused a lot. Yet, it is a nice study. In the below I generously borrow from a sceptical website that is more negative about the study than I am, but also seems to have actually missed the main point in the findings if you look carefully.
The authors randomly assigned 600 villages in rural Bangladesh – comprising more than 300,000 people – to one of two groups: an intervention group and a control group.
Villages in the intervention group received an eight-week mask promotion campaign, which involved distribution of masks, promotion of masks in public spaces, and role-modelling by community leaders (including imams at local mosques). Villages in the control group did not receive any interventions.
The main outcome variables were measures of seroprevalence. Using phone and in-person surveys, the researchers obtained data on the number of people who experienced COVID-19 symptoms after the intervention. They then collected blood samples from some of those individuals to gauge the number who were seropositive.
Overall, mask-wearing reached 42.3% in the intervention villages, compared to 13.3% in the control villages. What about the outcome variables? 7.6% of participants in the intervention villages reported COVID-19 symptoms, compared to 8.6% in the control villages.
And when the researchers zoomed in on those who reported COVID-19 symptoms and tested positive for antibodies, the seroprevalence was 0.68% in the intervention villages, versus 0.76% in the control villages. (Note: the figure in the chart below is ‘0.69’ because it is an adjusted value from a model.)
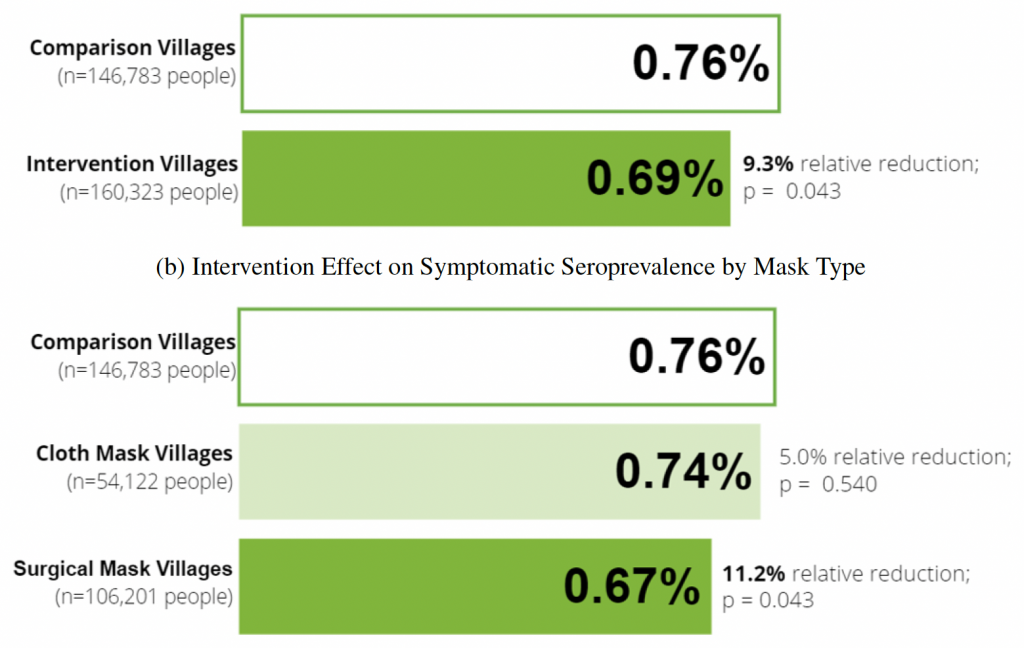
Among the intervention villages, some had been randomly assigned to get cloth masks, whereas others had been randomly assigned to get surgical masks. The researchers compared these two groups, and found that the reduction in seroprevalence was larger for the surgical mask group. They also found that the reduction was concentrated among individuals aged 50+ (see p.28).
Discussion
Let us take the findings at face value and trust them (I have no particular reason at this point not to trust that the authors did an honest job, for reasons I will make clear below).
The skeptical website discussing it points out that the study is looking at the effect of not just masks, but also a promotion campaign that will have included a lot more information than just on masks. Whilst that is true, I find that argument weak because that is true for any medical intervention that is hands-on and hence noticed by participants: what is tested is always not just the effect of a piece of medical equipment but also the effect of the whole hooha around it. That is also true for medical health interventions, happiness interventions, schooling interventions, etc. It does not take away from a finding that a whole package has some effect. It merely means that one cannot say for certain what element in the package did what, although one often can say something reasonable about that.
The much more important and key finding of the Sri Lanka study is that cloth masks clearly make no difference, either statistically or in size (from 0.76 to 0.74), despite a whole campaign around the use of cloth masks as well. That is a big finding and the one I think matters because it blows away mask studies that look at the supposed effects of cloth masks. This study is so big (300,000 people) that it also blows away all the small studies or happenstance studies (of the kind ‘we introduced masks and next day we had less positives in place X’). 300 villages is a big sample of places and people (50 times bigger than the Danish study) so it clearly is the new benchmark. So if I wanted to play propaganda I would say the Sri Lanka study proves cloth masks do nothing at all. I wouldn’t be surprised if that is exactly how it will be used.
The big difference the study finds between cloth mask effects and surgical mask effects, btw, also takes away from the argument that we are looking at the effects of village promotion activities or other information, because that effect would surely show up irrespective of mask-type. So it is more likely a true mask effect one is looking at with the surgical mask study. Its a smallish effect, but it is a clearly significant effect that at least conveys some potentially useful information (ie surgical masks might in some situations (villages) be a form of ‘focused protection’ for some groups).
If we then look at where we do find some significant and reasonable size effects, we thus need to look at the effects of surgical masks. They reduce the seroprevalence by about 11% (from 0.76 to 0.67). Another way to say it in the context of the length of the study (1-2 months) is to say these masks delay the spread of the virus by 1 week, a bit longer for the more at risk (the over 50).
Let me then make the economist point. How much do these masks cost? How many are used per day? How much would they help what type of villager? How much would the same resources improve health via other expenses? These are the questions that always need asking, particularly in a poor place where there are lots of cheap interventions to reduce child mortality, other infectious diseases, road fatalities, snake deaths (a big thing there), etc.
Interestingly, the study itself has tried to do this calculation and much of it is a quite reasonable calculation (their Appendix 1). They go over what the costs have been by type of village, coming to a ‘mid-range’ estimate of 100,000 USD per death from covid averted, using the costs of their own study. Kudos! They also say, quite reasonably, that doing this all at scale, so for the whole country, probably means costs would go down to about 16,700 USD (I find that calculation a bit optimistic on savings, but lets not quibble). They even helpfully tell us that in Sri Lanka, the statistical value of life is about 200,000 USD, meaning that that is what the average individual willingness to pay in Sri Lanka is to averted the loss of a whole life (though it will be way smaller in villagers where people are much poorer on average than in the cities). Then, unfortunately, they make two mistakes in one go by comparing the 16,700 to the 200,000 number: they presume individual willingness to pay is the same as what a government (who would do the ‘at scale’ intervention) should be willing to pay and that a covid-death amounts to a whole life lost (life expectancy in Sri Lanka is around 77). Both are rookie mistakes you see a lot these days.
For one, the average covid casualty does not have another 77 good years of life to go. In the West, it is more like 3. It is a bit hard to give a reasonable guess what it will be in a place like Sri Lanka, but given the actually quite high life expectancy there (only 2 years below the US!) and the unusually high numbers of covid-casualties for a poor country (probably around 0.1% of the population when the current wave is done), we are probably talking a very similar victim group in Sri Lanka as in the West. Let’s be generous and say 5 good years on average in Sri Lanka per covid-death. An individual willingness to pay for that in Sri Lanka would then be just below 15,000 USD (almost the same as average income for 5 years). So that would mean close to parity. However, individual willingness to pay is about 2.5 higher than government marginal productivity of health expenses in the West, simply because governments are much more health-productive than individuals: governments produce healthy years for a lot less than individuals are willing to pay for them. So the opportunity costs are far higher than the statistical value of life: if one is going to make the ‘at scale’ argument about costs one also has to use the ‘at scale’ opportunity costs, so not individual willingness to pay but marginal cost to the government of producing a year of good life. Applying those two insights, we are looking at a cost to benefit ratio of 2.5 to 1.
Moreover, of course, the authors do not take the long view on the dynamics of the virus and hence build into their assumptions the notion that avoiding infection in one wave means victory forever. As we have seen pretty much everywhere, that is a bit of an unwarranted fantasy: the virus keeps coming back in variants and such. So avoidance in one wave buys a bit of time but not a whole 5 good years (ie all that a would-be victim still has left on average). Hard to know how much postponement buys, but as a guess (based on the timing between waves so far), its more like a year, maybe 2. That brings the cost to benefit ratio up to 5 to 1.
So perhaps one can find parity for the absolutely most vulnerable, but unlikely for a whole community. And that for a place where masks then are about 5 cents per pop.
I did have a look at some of the hart group stuff on some of the obvious targets. Some of the stuff I agree people need to argue about more (childhood vaccinations, vaccine passports etc.) although I doubt they will in parliament.
Other stuff looked like cherry picking to me. For example compare:
https://www.hartgroup.org/promising-treatment-options/
with
https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD015017.pub2/full
I have a particular interest in ivermectin as there are several large trials underway to settle the question, so I had a look at your links.
One thing is the date of publication. The Hart advice you linked to was written at the end of March whilst the review you point to was end of july, so its a bit unfair to ask the march advice to contain the july information(the Hart people are not constantly updating). If you then look at the swpr website, which was updated in the last 2 weeks, you will find they discuss trial results from even later (August) and also point out that some of the negative ‘reviews’ have simply left out the positive studies (which at first glance is also what the review you sent you seems to do).
So on swpr (https://swprs.org/the-ivermectin-debate/) they give the following update:
seems pretty reasonable to me, conrad. Indeed, both the review you linked to and the swpr site announce that big trial results are coming in soon, that ivermectin is clearly no wonderdrug, and that the evidence is very poor at the moment.
in addition to that, the swpr is good at the politics of it all. So on the invermectin stuff they note the various fraudulent positive studies (!), discuss some of the limitations of the small trials (which are what the cochrane reviews mainly look at) but also slip in this gem on the issue of censorship (with links on their website):
A vaccine alliance buying google ads to play down a cheap competitor? Big Tech censoring those supporting a cheap drug widely used in poor countries? Its what an economist expects. Its the information world we now live in.
Yes I saw that about the fake positive results. People should be in the least case fined for stuff like that (and fake negative results too). Fake results in social psychology just add to junk. Fake results like that kill people and we don’t want to end up like China where I have seen estimates that 90% of clinical trials are fake, otherwise no-one will believe anything, and you couldn’t blame them.
The big trials will be interesting — although the likely problem for anti-virals will be that even if they do work, they will tend to work best when you use them really early, which those guys noted so it will be less useful for covid given the time-course. This is true of the current influenza ones too. Hopefully we will be lucky as we were with the vaccines and their high efficacy. I possibly also falsely believe the stem-cell stuff released by Mesoblast has the same problem with needing to be used really early.
I imagine the other problem is that they willlose efficacy over time quickly if they are used massively as the virus mutates (e.g., if they are given to people likely to catch the virus that don’t want to catch it), which happened to early influenza anti-virus drugs. So they won’t be a good cheap solution forever even if they do work.
Obviously the other stuff those guys mention which appears related to general health (getting proper vitamins and minerals), is a no-brainer, but it goes into your category of censored stuff because you don’t see it in the news presumably because there is not much money to be made from it.
Paul is there a estimate of just how many discarded masks have gone to landfill or street litter by now? And for the cost of all those masks?
several estimates doing the rounds John, ranging from 3 billion per day up to 10 billion per day.
Harder to know how much they cost as they are produced by many different manufacturers, some more expensive whilst others quite cheap. It has to be something in the order of 1 billion dollar per day though, making the industry into a 300-500 billion industry. That is a lot of political power on the side of continued mask usage and hence continued emergency.
Presumably that’s seen by many as a positive not a negative (it seems similar to the fast fashion stuff). New industries = more jobs, more consumption and more trade.
it is activity, certainly, and as such part of GDP. Yet, tax advisers and polluting mines are part of GDP to but it doesnt make their activities useful. Or clean. To judge that, we need a measure of whether the products and services created and promoted by this activity is good for society. Dare I say, one needs a measure of wellbeing….
We have had about a month where we have had to mask when walking down the street (as well as indoors in say the supermarket etc). Our ‘consumption’ of masks and spend they are surgical) has gone up a lot . I’d guess that over the past 18 months in Melbourne the number of discarded masks and spend would be astronomical.
BTW The requirement to wear a mask when walking down a near totally deserted, country town street does take the biscuit for , pointless.
And strictly speaking I’m supposed to mask when “working outdoors “ I.e. when I am completely alone and the nearest human ( apart from my wife) is typically ks away…
I am looking forward to your new book, Paul, and I watched the Germans interviewing one of your co-authors, Gigi Foster, on corona-ausschuss.de but I think you and Cameron Murray identified the underlying problem in Game of Mates. There is no independent analysis. Everybody has skin in the game. Regulatory capture is the technical term but corruption is a reasonable translation. The revolving door between Wall Street and Treasury is bad enough but when medical science falls into the same trap it is a matter of life and death. Quis custodiet ipsos custodes? Nobody.
British psychologists Gary Sidley is interesting on masks and when it comes to ivermectin and outpatient treatment it is worth listening to Vladimir Zelenko who wrote the letter to Trump. In a recent interview he said the protocol did not matter so much as when it is administered and to whom.
“when medical science falls into the same trap it is a matter of life and death”
exactly right. The medical ‘authorities’ too are now proving to be a huge problem. Those who run national health services or private health services too have an incentive to milk a health problem for all its worth, and they are doing so big time. Its part of the major governance problem our societies now face. That problem is becoming more and more visible to many people though, so I do think awareness is coming, which is a necessary step to real reform.
I share Paul’s scepticism with respect to masks. Placebo effects might be important but simply put most people don’t wear them properly.
I did however see one study that offered positive support – in today’s Age. I have not checked it out.
https://www.theage.com.au/world/asia/researchers-say-study-ends-debate-on-masks-shows-they-limit-covid-spread-20210902-p58o2w.html
I saw that too. Whilst it might well be entirely reasonable (I haven’t read the paper), it does show media bias — we didn’t find out about relatively similar studies that didn’t find any differences on the front page.
I suspect proper usage is important as Paul notes above and there are vast differences between groups. When I used to work in Asia, people typically wore the disposable ones, didn’t fiddle with them, took them off and threw them out correctly etc., entirely unlike here (including myself, despite knowing better). In places like Bangladesh there is also a big cost to getting sick given the limited healthcare, so I suspect people would try harder not to get sick and that might well mean using them properly, especially given they were giving the masks out for free and presumably giving information about using them.
Thanks for this article, pf.
As you may remember, I made comment quite independently quite some time ago on the relative sizes of the C-19 virions (15-100 nanometres) to even N95 mask mesh (>300 nanometres). A major manufacturer of the N95 masks (3M) even stamp “Not Effective for Viral Control” on the box.
Yet almost all Govts and medico bureaucracies insist on them. Control, of course, with some hopeful measure of panic control (ie. people may feel safer – certainly, the aggressive dobbing of those without masks supports this). These masks reduce individuality by covering expression, muffling speech and hiding faces; a robotic greyness is presented.
A few weeks ago, NSW suddenly decreed and aggressively enforced mandatory mask wearing outdoors – even in a vast empty paddock 1000km out of the cities. When questioned, the Chief Health Officer stated that there was no medical basis to this. The police had requested it to make it easier for them to spot likely dissenters. This is just the inverse of sewing yellow stars on coats – and done for exactly the same purpose. Identifying people in public streets without masks as dissenters is made so much easier.
And this is a result (warning – unpleasant viewing):
pic.twitter.com/vLKbxE1G5L
It is an important point, Ian. One of the many horrible aspects of fascism is the way it degrades the police, making them the enemies, rather than the servants of the people. Australia today is full-on Germany 1932-33.
Most of this is wrong.
Ivermectin does not work as a treatment for coronavirus, which is why the only major study into its use has been withdrawn. Medicine that works does not rely on made-up evidence.
https://ebm.bmj.com/content/early/2021/05/26/bmjebm-2021-111678
The group which you cite also still (!) supports the use of hydroxychloroquine. Again, the author of the only study suggesting the drug works has spent the last six months viciously harrassing and vilifying a scientist who proved he made it all up. Needless to say, real medicine does not rely on fake evidence or intimidation to prove it works. The reason Didier Raoult has resorted to that is because it doesn’t.
https://www.theguardian.com/world/2020/nov/12/covid-professor-didier-raoult-hydroxychloroquine
Outside of those two fabricated studies, there aren’t really any high-quality studies that show either drug works.
https://ebm.bmj.com/content/early/2021/05/26/bmjebm-2021-111678
Outside dexamethasone, and ventilators, we do not have any scalable, affordable drug that can cure or even treat COVID-19. Your group recommend monoclonal antibodies, which is fine, but patients certainly should not expect the taxpayer to pay for their extraordinarily expensive treatment for a very easily avoidable virus. Also, anyone who refused to get a vaccine because it was only approved under an emergency procedure, or who won’t get one now due to lack of long-term studies, should be flatly refused the antibodies, which are far worse on both fronts.
Many who use and abuse hydroxychloroquine and ivermectin do so as a way of virtue signalling their commitment to white supremacy and their fealty to Donald Trump as a human being and a symbol of that idea. They’re willing to sacrifice their health to the cause. I’m not sure why anyone who isn’t would bother.
By contrast, universal masking does work. There’s plenty of evidence. There’s just no need to pretend.
https://www.pnas.org/content/118/4/e2014564118
https://www.theage.com.au/world/asia/researchers-say-study-ends-debate-on-masks-shows-they-limit-covid-spread-20210902-p58o2w.html
I approved this comment even though I thought it a borderline case. Yet, it nicely illustrates what we are now up against: bland statements without real analysis simply claiming authority, refusing to apply the same concept of proof for lockdowns (show me the RCT!). Since the cheap drug ivermectin is used in 20 developing countries (and counting) I particularly found your statement on who advocates them interesting:
Right. How revealing. Sounds to me like the phrase used by someone who doesnt know much about non-white people in 20 developing countries.
The reason you have cited no evidence to support your position that the Trump cures work is because they do not.
As a reporter, Andrew, I look to sources at the coal face and in the Covid case that means doctors working to keep their patients alive. We have the first-hand testimony of such dedicated doctors as Zelenko, Pierre Cory, McCullough and many others who are not difficult to find speaking to the camera. When it comes to data on ivermectin, Dr Tess Lawrie has a compilation. I wonder where you are coming from, Andrew. As for data on the dangers of the vaccines, even the most conservative sources such as the British Yellow Card system should be enough to stop the vaccination campaign.
One could exactly the same thing about acupuncture.
“could say”
I just find the double standard extraordinary. You’re happy to accept the use of some VERY sketchy, almost completely unstudied drugs on the honesty system, with no evidence but the say so of some fairly sketchy doctors, many of whom have a direct, personal interest in the outcome. You’re happy to accept this even if the drugs – for instance, monoclonal antibodies – are approved on an emergency basis, have not been subjected to long-term studies and so on. You’re also happy to wave away the proven side effects of ivermectin, monoclonal antibodies and so on. But for probably the most studied drugs in human history, the coronavirus vaccines, it’s always the literal handful of negative cases, the supposed lack of evidence, this, that, or something else that is decisive.
Here’s a super easy rule: if there’s loads of evidence for one drug and no evidence for another, and you take the second one because you consider use of the first one unfounded, your concerns are pretextual.
Do you really want to argue with doctors treating thousands of patients or with the scientist who invented the vaccines? Who on earth do you think you are, Andrew? The new consensus in the last few days from the top of the profession is that we are all going to be infected by the Covid-19 virus much as we all catch a cold from time to time, so there is no need for the sort of mass testing we hear about every day on the news broadcasts in Australia.
Whether we get sick and die from the virus will depend on our general state of health, known in the trade as co-morbidities. Individuals have a decision to make. Are they at greater risk from the virus or from the vaccine? I see no room here for politicians or bureaucrats and certainly no role for the police or armed services.
Even the most avid vaccine promoters acknowledge that fully vaccinated people can still be infected by the virus and can still pass it on to others so there is no case for mandatory vaccinations. It is a matter for doctor and patient to discuss. This is the Nuremberg Rule — informed consent.
If it’s an appeal to authority you’re after, all I have to do it point at the TV to completely trump yours. Literally the highest authorities in medicine as one say you’re completely wrong about everything.
Also the “scientist who invented the vaccines”, Robert Malone, didn’t invent the vaccines.
Malone tells the story in a superb address on 10 August to the Liberty Forum of Silicon Valley. The same date was a day of infamy for the Australian Labor Party in Canberra. Ramesh Thakur tells the story in the Australian edition of The Spectator, 21 August.
I imagine the main case for mandatory vaccinations is that the unvaccinated people will tend to get sick and fill the hospitals and ICU wards, hence displacing those that need to go there for other reasons. In addition, more recent evidence suggests that rather unsurprisingly, they will be at a far greater risk of getting long covid. When they get that and become unemployed, the government will then have to pick up the tab for their unemplotment/disability benefits.
As it happens, I personally don’t think that justifies mandatory vaccines, but I’m sure many people do (especially those that work in the hospitals). Alternatively, annoyance measures like we use for smoking are probably worthwhile.
Vaccination also reduces the reproduction number, both by reducing the number of vectors for the bug and also the rate at which they spread it. At a high enough level, the bug just becomes the flu.
well, Andy Messenger (a messenger?), You will find on this website that if you want to really engage we do insist on fairly courteous language, reasoned positions (so not just ‘it is true because of link X’), and some degree of presumption of fidelity (so those we disagree with are not assumed Trump supporters unless that is truly clear). Name calling and tribalism are not something we like to engage in.
So, do you want to try again and re-write your stuff such that it can be engaged with? Otherwise it will be ignored.
If you read my comment I explicitly make the point that you are NOT a Trump supporter; hence my failure to understand your commitment to a group pushing Trump fake-cures for the bug. With a Trump supporter the explanation is simple; white supremacy. I don’t understand your position, which is neither a commitment to evidence nor white supremacy.
Needless to say I do not find the honesty system, faked research or other fraud to be compelling. By contrast, vaccines are extremely well-evidenced, probably the most well-evidenced treatments for any virus ever in the history of medicine. I also find the numerous contemporaneous double-blind and large-scale studies and other evidence into mask use against coronavirus to be convincing. I can show you several if you’d like. I don’t know why you do not find this convincing. I think it is pretexual, but I’m not going to say you’re making things up.
Hi Andrew. One of the many famous sayings from the poetry of the Trojan epic is “Timeo Danaos et dona ferentes.” One translation is – Beware of Greeks, especially when they are bearing gifts. A suitable modern saying is beware of politicians, especially when they are trying to frighten you.
I am half way through an essay by a Canadian scientist whom I heard about only this morning from a friend who is on Twitter. His name is Julius Ruechel and the essay is called “The Snake Oil Salesmen and the COVID Zero Con.” Have a read. You will need to set aside some time.
In Ruechel’s thesis, the Covid hysteria started as a racket by the pharmaceutical companies. The fascists, who are my interest as a political reporter, saw their opportunity and jumped on board.
You need to slow down with the assertions and try to take people as doing their best.
99% of the internet exists so you can slag off at people. ClubTroppo exists so you can challenge and discuss stuff with them.
It takes some skill, but you can learn it if you take a step back and take it more slowly.
I can’t see what this has to do with white supremacy, Andrew. The advice to Trump on hydroxychloroquine came from Vladimir Zelenko, a doctor in upstate New York at the height of the original Covid spread. The object of the exercise was to keep people out of hospital and out of the morgue. Doctors call the practice an outpatient protocol. Zelenko’s interview with Reiner Fuellmich and his colleagues on corona-ausschuss.de is a brief but fascinating insight into the history of the Covid-19 drama.
Hydroxychloroquine is widely used in Africa where most people are dark-skinned and is available over the counter in many countries where malaria is a problem, not so much in higher latitudes.
The last vaccine I took was for yellow fever when I was on the way to Africa. I sailed down the south-east trades to the Seychelles and flew to Nairobi. I would love to do it again but don’t like my chances.
I’m glad you asked!
This failed decision – which in my mine should have seen Trump impeached – is made up of two phenomenon.
To also address John R Walker below; even if Trump had been correct and hydroxychloroquine effective (it wasn’t) that really is irrelevant. The process behind drug development and approval does NOT solely rely on the personal opinions of an individual random doctor, who may or may not be self-interested and be acting in bad faith, who may or may not be qualified, who may or may not be right. Lots of doctors think lots of dumb stuff about medicine (lots of lawyers think dumb stuff about law, scientists about science…). No doubt you could find an MD to proscribe scores of drugs for hundreds of ailments that don’t work. Random-doctor-reckons as a procedure has a low accuracy rate in terms of identifying effective treatments.
Every president, but particularly Donald Trump, has a huge platform. They can convince thousands of people to do stuff – as Mr Walker says, to jump off a cliff. Doing as Trump does is part of your strong political identity. But presidents, particularly Donald Trump, are never going to have the time or inclination or in his case mental capacity or honesty, to judge correct from false. Also which doctors’ I-reckon goes in front of his eyes is pure chance; he’s not systematically going through all the I-reckons and figuring out which one seems best, and as I said, even if he were, he’s a big dummy who doesn’t know what he’s talking about, and is a huge corrupt liar^ who probably would use that knowledge to make a buck off it if he did.
So what we’ve got is a process which is essentially a high-failure rate alternative medical approvals process with no process for filtering bad faith medical advice, all based largely on the individual of the President plus chance, but which nonetheless affects thousands of peoples’ medical choices. Compared with our multi-billion dollar existing approvals process, which is flawed enough despite thousands of experts spending their lives working to gradually disprove all the dumb stuff doctors think about medicine and scientists about science, this seems suboptimal*.
Phenomenon 2:
There’s a really good book everyone should read about the Republican Party called ‘Dying of Whiteness’. Here it is:
https://www.basicbooks.com/titles/jonathan-m-metzl/dying-of-whiteness/9781541644960/
The thesis is that many Republicans put their racial and political identity ahead of their own health. The author literally asks a number of Republicans on their deathbed if they would access stronger healthcare systems in return for, eg, racial desegregation. (it’s more direct than this actually; literally policy x has put you on this deathbed, has no benefits, but by hurting some minority group, signals your commitment to white supremacy and its political party and its symbolic leader Donald Trump; do you still support policy x?). The answer is always yes, they would rather die, in fact.
The hydroxychloroquine thing, and the invermectin thing, is part of this dying of whiteness effect. Nobody is genuinely acting in the belief that this high-failure rate drug approvals process is better than the low-failure rate one. They are signalling, just like you might signal by wearing a red hat. Even at the cost of their lives.
Obviously there are many political implications of this sort of pathetic serf-like attitude by thousands of wealthy people in the first world. Freeing serfs in Russia was simple. But ending the serfdom of the mind will be more difficult.
* To be clear, the public absolutely should have a say in how drug approval functions. The current processes are genuinely quite flawed. But we should be trying to fix the system, not make it much worse by randomly adding half-assed second-guessing by assholes into it.
^ Evidence for this: Trump does not believe hydroxychloroquine works against COVID-19, and he does believe that vaccines do. I know this because he used the latter and did not use the former. He’s never going to tell anyone this openly, because, again, he is just about the worst man who has ever lived.
Andrew
Question for you :
if Trump had said that jumping out of a plane without a parachute was dumb , would you take that statement as proof that the opposite was true?
If you read my above comment you’ll see that I believe replacing the parachute safety regulator with Trump’s gut feeling isn’t a good move.
Was not asking you about the reliability of Trumps opinions etc, rather I was questioning you re the reliability (or predictability )of your opinions…
I’d suggest that is arguably the most boring and pointless logical fallacy of all. I genuinely don’t care and I doubt anyone else does whether you find my view interesting or not. I care if you agree, and if you do not, whether you have a decent argument for that view, or if it is just silly prejudice or something else unfounded. Given you’ve not made an effort to actually make that case I’d suggest it may be the latter. But I don’t want to assume! Feel free to make a rational case of some sort.
[notice of update]
I updated the post above with what is by far the best study I have seen so far on the effects of masks on covid-transmission, a Sri Lanka study with 300 villages and 300,000 individuals randomised over do-nothing, cloth-masks, and surgical masks, finding surgical masks do a bit but cloth masks do not. The study even tries its hand at a cost-benefit. Kudos, though they do make a few big mistakes right at the end (I do not think intentionally. Its just not clearly not their area of expertise. It is mine though so I walk the reader through the issues).
Mr Messenger, Andy,
Let’s see if we can find agreement on something quite particular. How about the fruitful way in which the CDC can be reformed? You argue the medical establishment and its systems for validation are deeply flawed. I could not agree more. You argue Trump is not the solution. Again, I could not agree more. So let me say what my proposal has been and lets see if you agree or have a better one?
My proposal (in troppo blogs and my book “the Great Covid Panic” is to have the head of the CDC (and perhaps even the top 10 of that whole organisation) appointed by a citizen jury of, say, 20 random US citizens from all walks of life. They get to decide on their own procedures, but are helped administratively (emails, websites). The purpose is to take politics and wealthy interests out of it, treating the members of the jury as civilians who can come to reasonable views. You can find further details on how to do this in my writings, but the idea and intent should be clear.
Do you have a better proposal?
There are so many areas of life where sortition could improve system function, and I very much agree that the US CDC and Australian ICEG, ATAGI and so on should be appointed through a sortition process. But I also think their decisions can be scrutinised on a weekly or monthly basis through a sortition-selected organisation like a jury. It’s important that the jury have access to a range of opinions from outside their agency (and it’s also important that each jury be separate and not coordinate with others – I reckon you have one for each department or independent body like the PHO, but also Defence, Treasury, the cops at state level, and so on). They should have the powers of a Royal Commission; any document, any member of staff; lying is perjury and so on. What do you reckon – overreach? Or do you have a selection panel and a day-to-day panel? It’s definitely 100% a vital element of oversight. (I think you also have a professional ICAC-style organisation at federal level that essentially acts like the cops for political decisions, except with a much lower standard of evidence – “the appearance of corruption”).
Upshot: I totally agree that sortition would break up the groupthink garbage, MD obsession, self-interest and incompetence that has infected public health in this country.
I think another element that is underreported is the effect of secrecy on decision-making. Secrecy is almost always bad for institutional effectiveness and is 100% always bad for accountability. It can still be necessary, of course; we don’t want spies’ names to be public, for instance. But we should 1) drastically reduce the range of justifications for making a file secret and publish all others on an easily-accessible website, and completely do away with Cabinet secrecy and 2) SEVERELY punish public servants responsible for over-classification. A public servant should face the exact same punishment for false classification as they might for selling classified information to a Russian spy – decades in prison, social opprobrium and so on. A public servant who leaks improperly classified information – witness K and Bernard Collaery for instance – should be required to be instantly promoted, guaranteed tenure and paid a bonus by law, and there should be automatic rules requiring any in-office bullying be severely punished, up to and including sacking. If “health advice” was public, I think governments would have made much better decisions. Sortition can aid both of these processes as well. It’s the best!